The Process of Conception
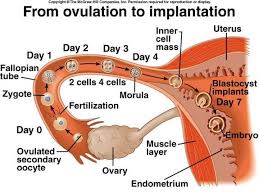
In order to understand the fertility tests and treatments you may be offered, it is important to understand how conception naturally occurs. First, your ovary must release (ovulate) an egg. This usually occurs once a month, approximately mid-way through the menstrual cycle.
The egg must be picked up by the fallopian tube. Sperm must travel through the vagina, into the uterus, and up into the fallopian tube in order to fertilize the egg. The fertilized egg, or embryo, then travels down the fallopian tube to the uterus, where it implants in the uterine lining and develops.
A problem in any part of this process can lead to infertility.
Fertility Factors
The Male Factor
In approximately 40% of infertile couples, the male partner is either the sole or a contributing cause of infertility. Therefore, a semen analysis or sperm test, is important in the initial evaluation.
To prepare for a semen analysis, your partner will be asked to abstain from ejaculating for at least 48 to 72 hours. The semen specimen is examined under a microscope to determine the count (number), motility (movement), and morphology (appearance and shape) of the sperm.
Other hormonal and genetic tests may be recommended as well depending on the type and severity of abnormalities found.
Several factors may affect sperm production and male infertility:
- Current or past infection of the testes.
- Growth of the testes
- Side-effects of some medicines and street drugs.
- Certain hormonal problems.
Treatment for male factor infertility may include antibiotic therapy for infection, surgical correction of varicocele (dilated or varicose veins in the scrotum) or duct obstruction, or medications to improve sperm production. In some cases, no obvious cause of poor sperm quality can be found. Intrauterine insemination (IUI) may then be recommended.
Female Factors
The Ovulation Factor
Problems with ovulation are common causes of infertility, accounting for approximately 25% of all infertility cases.
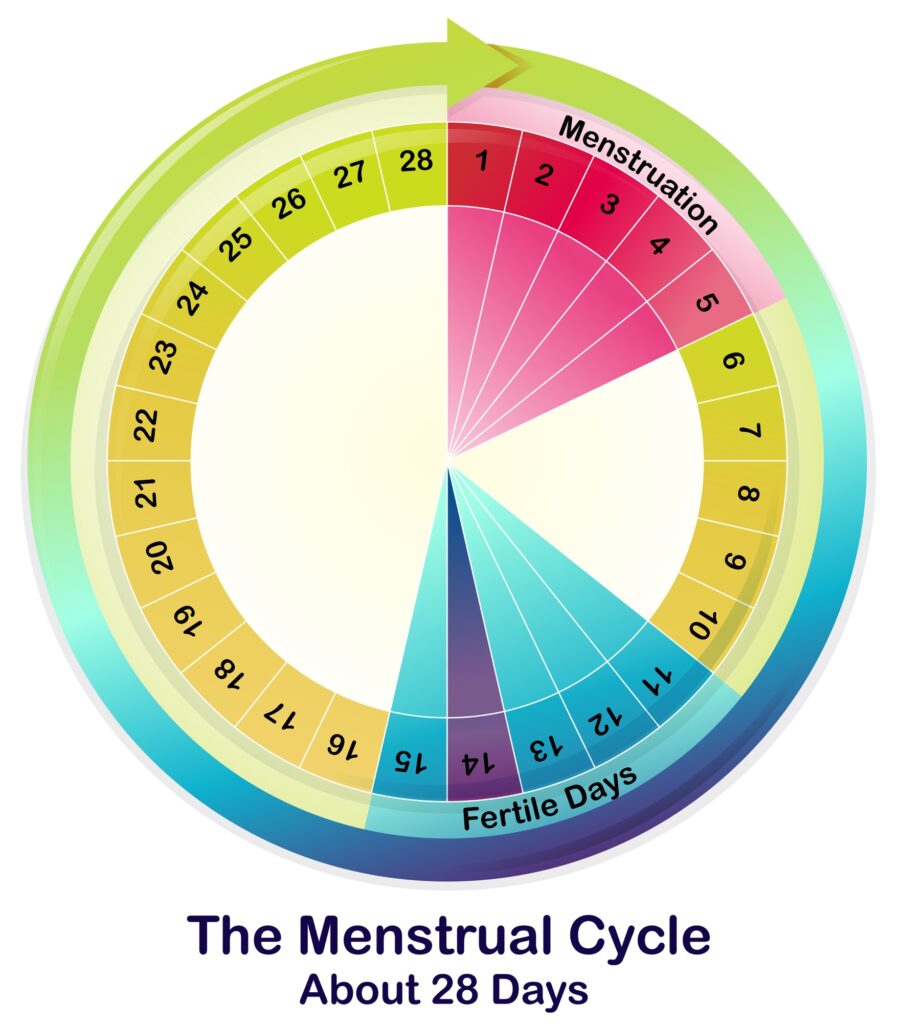
Ovulation involves the release of a mature egg from one of your ovaries. This usually occurs every month, about midway in your menstrual cycle. After ovulation, the ovary produces the hormone progesterone. During the 12 to 16 days before menstruation begins, progesterone prepares the lining of your uterus into an optimal environment for implantation and nurturing of the fertilized egg.
If you have regular menstrual cycles, you are probably ovulating. Cycle lengths of approximately 24 to 34 days ovulatory. If you only have a period every few months or not at all, you are probably not ovulating or are ovulating infrequently.
If you are not ovulating, your doctor may order special tests to determine the reason and then prescribe certain drugs to induce ovulation. Your medical history and physical exam will help determine which tests are appropriate. Both oral and injectable medications are available to help induce your ovulation.
The Tubal Factor
Because open and functional fallopian tubes are necessary for conception, tests to determine tubal openness (patency) are important. Tubal factors account for about 35% of all infertility problems.
A special x-ray called a hysterosalpingogram (HSG) can be performed to evaluate the fallopian tubes and uterus. During an HSG, a special fluid (dye) is injected through your cervix, fills your uterus, and travels into your fallopian tubes. If the fluid spills out the ends of the tubes, they are open. If the fluid does not spill, then the tubes are blocked.
If the tubes are found to be blocked, scarred, or damaged, surgery can sometimes correct the problem. But surgery does not guarantee that the tube, even if opened up or cleared of scar tissue, will function properly.
The Cervical/Uterine Factor
Conditions within the cervix, which is the lower part of the uterus, may impact your fertility, but they are rarely the sole cause of infertility. It is important for your doctor to know if you have had infections, prior biopsies or surgeries of the cervix, or abnormal pap smears.
The HSG test, often used to investigate the fallopian tubes, can also reveal defects inside the uterine cavity, which is the hollow space inside your uterus where an embryo would implant and develop. An HSG is typically done after your period stops and before ovulation. Possible uterine abnormalities that may be identified include scar tissue, polyps (bunched-up pieces of the endometrial lining), fibroids, or an abnormally-shaped uterine cavity. Problems within your uterus may interfere with implantation of the embryo or may increase the incidence of miscarriage.
The Peritoneal Factor
Peritoneal factor infertility refers to abnormalities involving the peritoneum (lining of the surfaces of your internal organs) such as scar tissue (adhesions) or endometriosis, a condition where tissue that normally lines the uterus begins to grow outside the uterus.
This tissue may grow on any structure within the pelvis including the ovaries and is found in about 35% of infertile women who have no other diagnosable infertility problem.
Endometriosis is found more commonly in women with infertility, pelvic pain, and painful intercourse. Endometriosis may affect the function of the ovaries, your ovarian reserve, the function of the fallopian tubes, as well as implantation..
The Age Factor
Fertility declines with age because fewer eggs remain in your ovaries, and the quality of the eggs remaining is lower than when you were younger.
Blood tests are now available to determine your ovarian reserve, a term which reflects your age-related fertility potential. In the simplest of these tests, the hormones follicle-stimulating hormone (FSH) and estradiol are tested in your blood on the second, third, or fourth day of your menstrual period. An elevated FSH level indicates that your chances for pregnancy may be lower than routinely expected for your age, especially if you are age 35 or older. Abnormally high FSH-levels do not mean that you have no chance of successful conception. However, they may indicate that success rates may be lower, that more aggressive treatment may be warranted, and/or that higher medication doses may be needed.
Older women tend to have a lower response to fertility medications and a higher miscarriage rate than younger women. The chance of having a chromosomally abnormal embryo, such as one with Down syndrome, also increases with age. Because of the marked effect of age on pregnancy and birth rates, it is common for older couples to begin fertility treatment sooner and, in some cases, to consider more aggressive treatment than younger couples.
Unexplained Infertility
In approximately 10% of couples trying to conceive, all of the above tests are normal and there is no easily identifiable cause for infertility. In a much higher percentage of couples, only minor abnormalities are found that should not be severe enough to result in infertility. In these cases, the infertility is referred to as “unexplained”.
Couples with unexplained infertility may have problems with egg quality, fertilization, genetics, tubal function, or sperm function that are difficult to diagnose and/or treat. Fertility drugs and IUI have been used in couples with unexplained infertility with reasonable success.
Continue reading about Treatment of Infertility